
Cervicogenic Headaches
What is a Cervicogenic Headache (CH)?
‘Cervico’, meaning ‘of the cervical spine (neck)’ and ‘genic’, stemming from the Latin word genesis, which means ‘create’, gives us a definition for a cervicogenic headache – a headache created by the neck.
Commonly a CH will present as a gradual, dull, achy pain which is often unilateral (one-sided) but occasionally bilateral (two-sided). Often people will describe it as a pulling or gripping feeling, and often will describe the feeling of a tight band around the head.
Commonly pain may travel between the head and neck to active ‘trigger points’. Trigger points are commonly referred to as knots. They are basically an area of the muscle that is tighter than the remainder of the muscle. Some common trigger points associated with CHs are underneath the occiput (back of the head), the upper trapezius (back of the neck into shoulders) and around the edges of the shoulder blade/s.
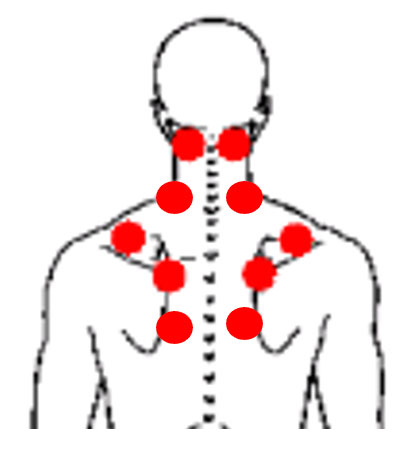
Figure 1 - Common Trigger Points associated with a Cervicogenic Headache
What causes a Cervicogenic Headache?
A CH is caused by abnormalities of the joints, muscles, fascia or neural structures in the cervical region (neck). It can be caused from one of these structures individually or by a combination of affected structures.
Some elements that can cause these structural abnormalities include; poor movement patterns, poor and/or prolonged posture (head forward position) and repetitive strain.
A prime example of how a majority of people get a CH headache is when an individual is working a desk job and looking at a computer screen all day with poor posture and not changing positions regularly.

Figure 2 – A Prime example of poor posture, this guy definitely has Cervicogenic Headaches!
Often weakness and impaired control of the in the cervical flexors (forward benders) and extensors (backward benders) is a contributing factor that leads to CH headaches also.
Stress is a massive contributing factor to CH headaches. This is the case because as we get stressed everything changes - we forget to take deep breaths from our diaphragm. As a result, our neck muscles take over our breathing and tend to shorten/tighten. So if you have a CH, try to find ways to de-stress and relax!
How do we fix a Cervicogenic Headache?
A multi-faceted treatment approach when dealing with CH can promote good recovery rather than just one element in isolation. A combination of all the below elements when going through Physiotherapy or Chiropractic rehabilitation is key to good outcomes.
Manual Therapy
Massage, trigger point release and joint mobilisation of the neck and head performed by a Physiotherapist or Chiropractor can lead to reduced CHs.
Dry needling
Needles being placed into trigger points can relieve muscular tension and reduce pain.
Traction
“Mulligan’s Traction Technique added to traditional treatment (heat, transcutaneous electrical nerve stimulation (TENS), and deep cervical flexors strengthening exercises) was more effective than traditional treatment alone in increasing the upper cervical rotation ROM to the affected side… Traction revealed a significant improvement in all outcome measures.” (Khalil, Alkhozamy, Fadle, Hefny, & Ismail, 2019)


Stretching and Posture correction
Stretching tight neck muscles, correction of posture and promoting regular changes of position every 20-30 minutes can be hugely beneficial in reducing CHs.
De-stressing and relaxation techniques
Any activities to destress can help CHs, these can include deep breathing techniques and meditation.
References:
Power, L., Murray, K., & Szmulewicz, D. (2020). Characteristics of assessment and treatment in Benign Paroxysmal Positional Vertigo (BPPV). Journal Of Vestibular Research, 30(1), 55-62. doi: 10.3233/ves-190687
Oron, Y., Cohen-Atsmoni, S., Len, A., & Roth, Y. (2015). Treatment of horizontal canal BPPV: Pathophysiology, available maneuvers, and recommended treatment. The Laryngoscope, 125(8), 1959-1964. doi: 10.1002/lary.25138
Shigeno, K. (2017). Positional Down-Beating Nystagmus caused by a variant of Posterior-canal BPPV or Anterior-canal BPPV. Equilibrium Research, 76(6), 684-691. doi: 10.3757/jser.76.684
Bhandari, A., Kingma, H., & Bhandari, R. (2021). BPPV Simulation: A Powerful Tool to Understand and Optimize the Diagnostics and Treatment of all Possible Variants of BPPV. Frontiers In Neurology, 12. doi: 10.3389/fneur.2021.632286
Aso, S., Yasumura, S., Asai, M., Shojaku, H., & Watanabe, Y. (1995). The Effect Of Epley's Maneuver On Benign Paroxysmal Positional Vertigo(BPPV). Equilibrium Research, 54(6), 547-552. doi: 10.3757/jser.54.547