
Gestational Diabetes
Diabetes in Pregnancy can be classified into two categories:
- Women who have Type 1 or 2 Diabetes Mellitus who fall pregnant, called Pre-Gestational Diabetes (Pre-GDM)
- Women who develops diabetes during a pregnancy, called Gestational Diabetes Mellitus (GDM)
In particular, this article is about gestational diabetes mellitus (GDM) which is when a woman is diagnosed with a glucose intolerance during pregnancy, usually during the 2nd or 3rd trimester. GDM affects 4.5% of all pregnant women(1) and in most cases it is a temporary condition. However, if not managed well it can have very serious and lasting consequences for both the baby and mother.

Uncontrolled GDM increases the risk of respiratory distress syndrome, premature birth, newborn death or stillbirth. Later on in life, it increases a child’s chance of developing type 2 diabetes and obesity. In mothers, gestational diabetes increases the risk of having a C-section, sustaining birthing injuries and developing type 2 diabetes in the future.
As rates of obesity and sedentary lifestyle grow, GDM numbers are also grow. Numbers in NSW have increased by 45% between the years of 1995 and 2005(2) and are set to continue rising. So what causes GDM? And how can it be treated?
What causes Gestational Diabetes Mellitus?
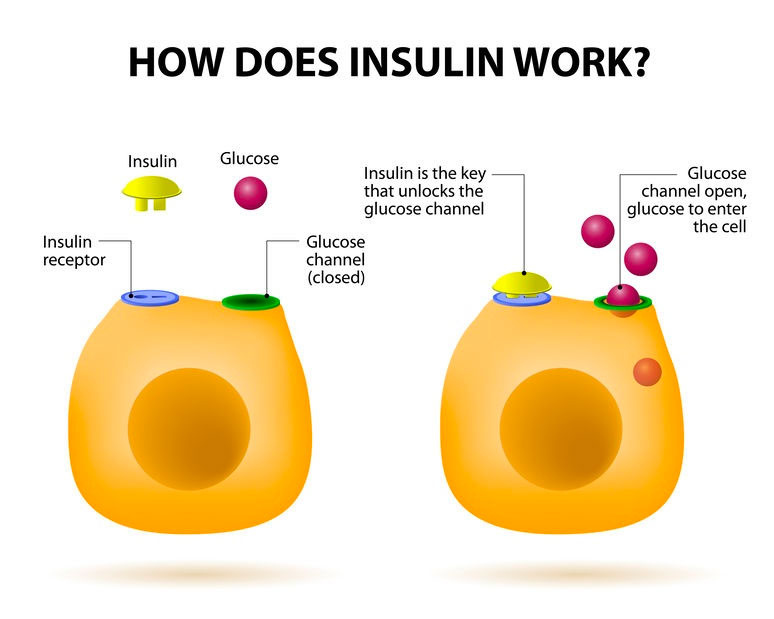
To explain GDM we need to know the relationship between the hormone insulin and glucose (i.e. sugar). All the cells of our body take in glucose from the bloodstream to produce energy. However, glucose cannot enter cells without the hormone insulin, which acts like a key to allow glucose in.
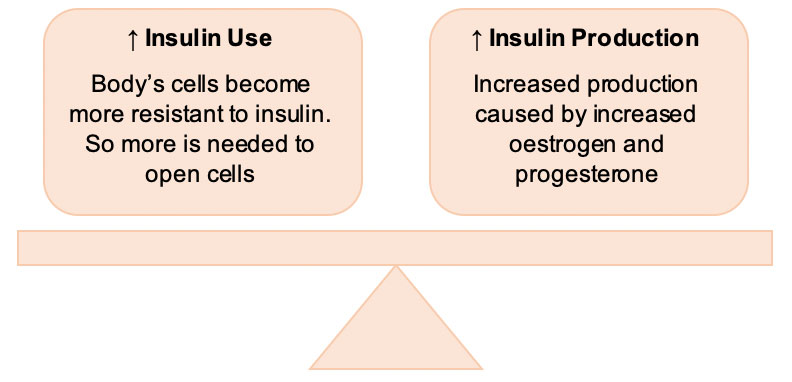
When a woman is pregnant there is an increased demand for glucose in the body, as a baby is growing in the womb. In a normal pregnancy, this causes both:
- The body’s cells to become more resistant to insulin. That is, more is required to open cells and allow glucose in.
- Increased production of insulin by the body caused an increased in pregnancy hormones, such as oestrogen and progesterone
This creates a balance between insulin use and production, and as such the body’s cells are receiving the glucose they need. GDM arises when this system is not balanced – either the body’s cells are too resistant to insulin, or body is not producing enough insulin. Both lead to an increased amount of glucose in the bloodstream and the high blood glucose level (BGL).
How do you treat Gestational Diabetes Mellitus?
The aim of treatment in GDM is to keep blood glucose levels (BGLs) as close to normal as possible. This may require a combination of:
- Dietary changes: monitoring and modifying intake of carbohydrates to avoid sharp spikes in glucose intake.
- Regular exercise: exercise (aerobic or strength-based) can decreased the body’s cells resistance to insulin. So less insulin required for glucose to be taken up by cells.
- Insulin therapy: to supplement the reduced levels of insulin in the blood, and restore balance between insulin use and production.

References
1. Shand AW, Bell JC, McElduff A, Morris J, Roberts CL. Outcomes of pregnancies in women with pre-gestational diabetes mellitus and gestational diabetes mellitus; a population-based study in New South Wales, Australia, 1998-2002. Diabet Med. 2008 Jun;25(6):708-15. doi: 10.1111/j.1464-5491.2008.02431.x. PubMed PMID: 18544109.
2. Anna V, van der Ploeg HP, Cheung NW, Huxley RR, Bauman AE. Sociodemographic correlates of the increasing trend in prevalence of gestational diabetes mellitus in a large population of women between 1995 and 2005. Diabetes Care. 2008 Dec;31(12):2288-93. doi: 10.2337/dc08-1038. Epub 2008 Sep 22. PubMed PMID: 18809630; PubMed Central PMCID: PMC2584183.